


Neuroscience




Disorders of Writing
Rhawn Gabriel Joseph, Ph.D.
AGRAPHIA
Disorders of Writing & Spelling
The inability and the loss of the ability to write and spell (when writing), is referred to as "agraphia" i.e. an inabiliy to form graphemes. Agraphia is a neurological disorder involving the loss of the ability to write.
The Neurology of Writing
There are a number of brain areas which interact and which are responsible for various aspects of the ability to write. Likewise, there are a number of theories which have been proposed to explain the ability to write, and the loss of writing ability.
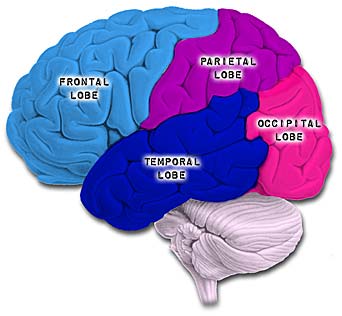
Broadly considered, the principle structures include the left frontal lobe (Exner's Writing Area and Broca's Expressive Speech area), the left temporal lobe (Wernicke's receptive speech area), and the superior and inferior parietal lobe. Exner's and Broca's area are implicated in the expressive aspects of writing, whereas the temporal and parietal lobe are involved in the comprehension of written words. However, the parietal lobe is also believed to program the frontal motor areas and to supply the anterior region of the brain with the grapheme equivalents of auditory language; i.e. converting or visual images sounds into written symbols.
Presumably the parietal lobe constructs the written-word images (probably via interaction with Wernicke's area) which and assists in converting these into graphemes. These motor-graphemes (or written word/letter images) are then transmitted to the left frontal convexity (i.e. Broca's and Exner's area) for grapheme conversion and motoric expression.
It has also been proposed that there are at least two stages involved in the act of writing: a linguistic stage and a motor-expressive-praxic stage. The linguistic stage involves the encoding of auditory and visual information into syntactical-lexical units--the symbols for letters and written words. This is mediated through the angular gyrus which thus provides the linguistic rules which subserve writing. The motor stage is the final step in which the expression of graphemes is subserved. This stage is mediated presumably by Exner's writing area (located in the left frontal convexity) in conjunction with the inferior parietal lobule.
Because different regions of the brain contribute to the ability to write, damage to these different areas, therefore, affect different aspects of the ability to write. Thus, there are different subtypes of agaphia, depending on which areas of the brain have been damaged. These subtypes are referred to as Frontal Agraphia, Pure Agraphia, Alexic Agraphia, Apraxic Agraphia, and Spatial Agraphia.
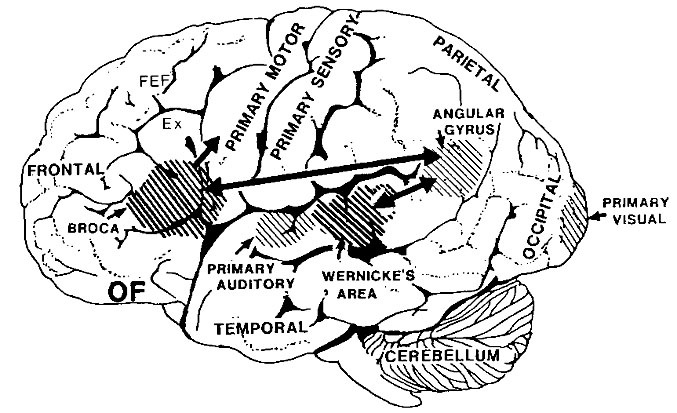
Exner's Writing Area is located within a small area along the lateral convexity of the left frontal lobe, and is adjacent to Broca's expressive speech area, and the primary and secondary areas controlling the movement of the hand and fine finger movements.
Exner's area appears to be the final common pathway where linguistic impulses receive a final motoric stamp for the purposes of writing. That is, Exner's area translates auditory-images transferred from the posterior language areas, into those motor impulses that will form written words and sentences.
Exner's area is very dependent on Broca's area with which is maintains extensive interconnections. That is, Broca's area also acts to organize impulses received from the posterior language zones and relays them to Exner's area for the purposes of written expression.
FRONTAL LOBE AGRAPHIA
Lesions localized to the left frontal lobe and Exner's and Broca's area typically result in disturbances in the elementary motoric aspects of writing, i.e. Frontal Agraphia. Frontal lobe agraphia, however, is sometimes referred to as Pure Agraphia. On the other hand, pure Agraphia has also been attributed to left parietal lesions (Basso et al. 1978; Strub & Geschwind, 1983). The similarity in symptoms is probably due to the fact that the inferior parietal lobe (IPL) transmits auditory-motor impulses to Broca's and Exner's area, and assists in programing sensory-motor movements.
In general, with frontal agraphia, grapheme (letter) formation becomes labored, uncoordinated, and takes on a very sloppy appearance. Cursive handwriting is usually more disturbed than printing, as cursive handwriting requires additional fine motor control. Cursive handwriting is also acquired at a later age, and is thus more likely to be more severely disrupted than printing which is (comparatively) an older and more ingrained skill.
With frontal agraphia, the ability to spell is often affected. Patient's may not be able to spell correctly even if given block letters--particularly if the left IPL is also damaged.
However, with frontal agraphia, primarily, it is the ability to properly form letters and words that is disrupted.
Predominantly, with frontal lesions, and thus frontal agraphia, there is a disturbances in grapheme selection. That is, the wrong letters may be chosen, and the patient may seem to have "forgotten" how to form certain letters. They may write the wrong letter--which in turn makes it appear that they have forgotten how to spell. Those with frontal agraphia may also abnormally sequence or even add unnecessary letters when writing.
In general, with a left frontal lesion, spelling and writing with both the right and left hand is severely affected, and the left hand may be even more profoundly affected.
Patients with frontal agraphia, particularly if Broca's area is damaged, are unable to write spontaneously or to dictation. Writing samples are contaminated with perseverations (such that they write the same letter over and over) or the addition of extra strokes to letters (e.g. such as when writing an "m"=mmm).
Patients with frontal agraphia may be unable to even write their name.
PURE (PARIETAL LOBE) AGRAPHA
Pure agraphia is associated with frontal lesions, but is most commonly secondary to damage involving the superior and inferior parietal lobe (IPL). The IPL sits and the junction of the frontal, parietal, occipital, and temporal lobe, and assimilates and integrates complex auditory, visual, motor and tactile sensations so as to form those multi-modal images and concepts which are integral to the comprehension and expression of human language.
With IPL damage, patients have difficulty programming those movements necessary to form written words, such that there is a loss of the ability select, form, and express, in writing, words and sentences.
Patients with pure (parietal lobe) agraphia frequently misspell words, and may insert the wrong letters or place them in the wrong order or sequence when attempting to write. In contrast, reading, oral speech and the ability to name objects or letters are usually unimpaired.
Most commonly, pure agraphia is associated with lesions involving the superior and mid parietal regions of the left hemisphere; areas, 5 and 7 (Basso, et al. 2008; Vignolo, 2003), and/or the inferior parietal region (Strub & Geschwind, 1983). Patients are unable to write because the area involved in organizing visual-letter organization (i.e. the inferior parietal lobe) is cut off from the region controlling hand movements in the frontal lobe (Strub & Geschwind, 1983). However, according to Vignolo (2003), the posterior superior left parietal lobule (area 7) is crucial for the sensorimotor linguistic integration needed for writing.
It has also been argued that the sensory motor engrams necessary for the production and perception of written language are stored within the inferior parietal lobule of the left hemisphere. When this region is damaged, patients sometimes have difficulty forming letters due to an inability to access these engrams (Strub & Geschwind, 1983). Writing samples, therefore, are characterized by mispellings, letter ommissions, distortions, temporal-sequential misplacements, and inversions.
ALEXIC-AGRAPHIA
Alexic agraphia is a disturbance involving the ability to read (alexia) and to write (agraphia). Thus alexic-agraphia is a disturbance in the ability to decode and to encode written language.
Reading and writing may not be equally affected. Some patients may be able to recognize written letters, but are unable to form them. Some patients can form the letters, but are then unable to read them. However, even those who are able to read the letters or words they cannot write, began having difficulty as the words become longer or less familiar.
Patients with alexic-agraphia have generally have difficulty with spelling, even when block letters are employed. Thus the ability to spell, per se, is disrupted. (Marcie & Heilman, 1979).
Often alexia-agraphia is due to a lesion involving the left inferior parietal lobule and angular gyrus (Benson & Geschwind, 1969; Hecaen & Kremin, 1977). Because alexic-agrahia is associated with parietal lesions, it is also referred to as parietal lobe alexia. That is, rather than referred to as alexic agraphia, as patients who cannot spell are unable to write appropriately by definition, this condition could simply be referred to as alexia. However, what distinguishes alexic agraphia from alexia, is the disturbance of motor control which is not characteristic of alexia per se. That is, alexia is a loss of the ability to read, and is not related to motor abnormalities, as is the case with agraphia and alexic-agraphia.
APRAXIC AGRAPHIA
When a patient has difficulty sequencing their movements or performing skilled movements involving a series of steps, the disorder is referred to as Apraxia. There are subtypes of apraxia, and different aspects of this disorder are seen with frontal vs parietal lobe lesions--in which case the ability to write may also be severely disrupted. This latter condition is referred to as apraxic agraphia.
Because the patient is also apraxic, the ability to make gestures or complex patterned movements becomes abnormal such as those involved in writing is also deficient. That is, the ability to correctly temporally sequence hand movements is affected which interferes with the ability to write. The patient no longer knows how to correctly hold or manipulate a pen, or how to move their hand when writing. However, if given block letters, or if asked to spell out loud, they may be able to spell correctly.
SPATIAL AGRAPHIA
Right cerebral injuries can secondarily disrupt writing skills due to generalized spatial and constructional deficiencies. This is because the right half of the brain, although minimally involved in grammar and word selection, is dominant for almost all aspects of visual spatial functioning and orientation, including the ability to coordinate movements in space. This would include those fine motor movements involved in writing.
Hence, with right hemisphere lesions, particularly right temporal-parietal injuries, words and letters will not be properly formed and aligned even when copying. Patients may have difficulty writing sentences in a straight line, and/or letters may be slanted at abnormal angles. In some cases the writing may be reduced to a scrawl. In addition, patients may write only on the right half of the paper such that as they write, the left hand margin becomes progressively larger and the right side smaller (Hecaen & Marie, 1974). That is, they ignore the left half of visual space including the left half of the page they are writing on. If allowed to continue patients may end up writing only along the edge of the right hand margin of the paper.
Patients with right hemisphere lesions may tend to abnormally introduce spaces between letters within the words they are writing, particularly when writing cursively (i.e. cu siv e ly ). This is due to a failure to perform closure as well as a release over the left hemisphere (i.e. left hemisphere release). That is, whereas the right hemisphere performs closure, the left introduces sequences. If the right hemisphere is damaged, the left hemisphere acting unopposed begins to abnormally temporally-sequence and thus produce sequences separated by spaces, when writing. However, abnormal sequencing can also result from left hemisphere lesions
APHASIA & AGRAPHIA
Aphasia is a disorder of receptive and expressive language, involving loss of comprehension, or loss of the ability to speak, or both.
Although every patient with agraphia does not necessarily suffer from aphasic abnormalities, every patient who has aphasia has some degree of agraphia. Thus patients with aphasia always suffer from some degree of agraphia, though patients with agraphia do not always suffer from aphasic disturbances.







DVD - Brain Lectures
Six Lectures
3 DVD set = $29.95(+ shipping)
Pay By Paypal.com
DVD 1: Brain Overview
DVD 2: The Left Hemisphere, Brainstem, Midbrain, Thalamus
DVD 3: The Frontal Lobes: Frontal Lobotomy, Memory, Aphasia, Paralysis
DVD 4: The Parietal Lobes: Touch, Body-in-Space, Body Image, Hemi-Neglect, Phantom Limbs,
DVD 5: The Temporal Lobes: Language, Memory, Aphasia, Hallucinations, Face Recognition
DVD 6: The Limbic System: Amygdala, Hippocampus, Hypothalamus, Sex, Emotion, Memory, Stress, PTSD, Hallucinations