





Rhawn Gabriel Joseph, Ph.D.
BrainMind.com
SELF-DECEPTION AND CONFABULATION
Dr: "Give me your left hand!" (The patient presents the right hand. The doctor takes hold of the right hand.)
Dr: "Give me your left hand!" (The patient looked puzzled and did not move.)
Dr: "Is there anything wrong with your left hand?"
Pt: "No, doctor."
Dr. "Why don't you move it, then?" (The left hand was held before her eyes.)
Pt.: "I don't know."
Dr: "Is this your hand?"
Pt: "Not mine, doctor."
Dr: "Whose hand is it, then?"
Pt: "I supposed it's yours, doctor."
Dr: "No, it's not. I've already got two hands. Look at it carefully."
Pt. "It is not mine, doctor."
Dr: "Yes it is, look at that ring; whose ring is it?"
Pt.: "That's my ring; you've got my ring, doctor."
Dr: "Look at it--it is your hand.
Pt: "Oh, no doctor."
Dr: "Where is your left hand then?"
Pt: "Somewhere here, I think." (Making groping movements near her left shoulder.) (Adapted from Sandifer, 1946).
It can be said that a person has lied when he or she knowingly possesses the truth yet consciously attempts to deceive another person. However, it sometimes happens that a person half persuades themselves that the lie they have told is true and then behaves accordingly. In these instances it can be said that they have engaged in self-deception (Joseph, 1982, 1986, 1988).
Self deception is not uncommon among men and women, due in part to the manner in which the brain and mind are organized. That is, the language dominant left hemisphere is often unable to fully verbally comprehend or gain complete verbal access to non-veral and emotional impulses and non-linguistic knowledge sources, including memories, stored or generated in the right half of the brain or limbic system. Some impulses may also be partially or fully inhibited before reaching the language dominant left hemisphere by the frontal lobes (Joseph, 1999).
Because these different brain areas "speak" different "languages," information and impulses arising in, for example, the limbic system, may not be understood or properly translated upon reaching the left hemisphere which has difficulty comprehending and perceive emotional nuances. This is because the left hemisphere is specialized for perceiving, analyzing, and expressing words, sentences, temporal sequences, and mathematical concepts, and has difficulty with other forms of information which are processed by yet other areas of the brain.
Because only certain aspects of the original message may even be received in the language areas of the left hemisphere, this region of the brain is thus confronted with a gap or numerous gaps in the information it receives.
Nevertheless, because the left hemisphere is dominant for language, it provides the psychic foundation for the language-dependent aspects of consciousness, i.e. verbal consciousness. In consequences, if the verbal aspects of consciousness, that is, the language axis does not receive the complete message, those aspects which it does not receive remain essentially unconscious.
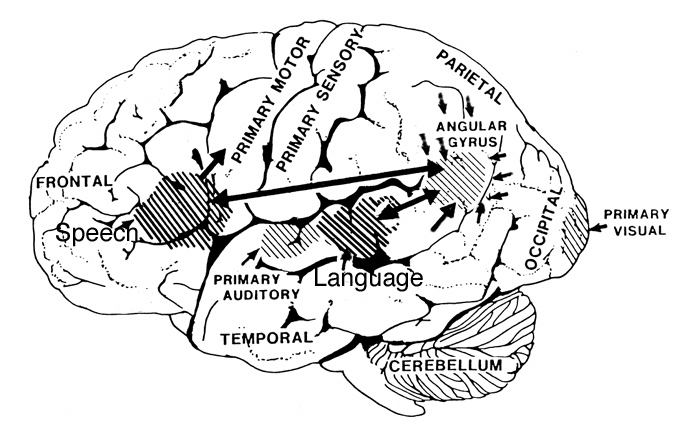
However, when confronted with a gap in its knowledge, the language axis (Broca's and Wernicke's areas and the inferior parietal lobe) will attempt to fill those gaps with related associations. In consequence, the message may be completely misinterpreted and the individual may confabulate and engage in what appears to be self-deception.
THE NEUROLOGY OF CONFABULATION: GAP FILLING
In contrast to self-deception, which is a "normal" aspect of human psychological functioning, confabulation is generally secondary to neurological immaturity or abnormalities, such as damage to the frontal or parietal lobes, or corpus callosum injuries or immaturity.
When the frontal lobes are compromised there is much flooding of the association and assimilation areas with tangential and irrelevant information much of which is amplified completely out of proportion to more salient details (Fischer et al. 1995; Joseph, 1986a, 1988a, 1993, 1996, 1999). Consequently, salient and irrelevant, highly arousing and fanciful information are received in the language areas and are expressed indiscriminantly. The normal filtering and inhibitory regulatory actions of the frontal lobes are disrupted and irrelevant information is mixed with irrelevant details and is expressed without concern for reality.
By contrast, when the parietal lobes are compromised, rather than flooding of the speech areas, there results a disconnection and information received in the Language Axis is incomplete and riddled with gaps (Joseph, 1986a). The language axis then attempts to fill that gap with relevant associations.
However, the larger the gap in the information received, the more irrelevant and confabulatory becomes the patient's speech. This also holds true regarding corpus callosum immaturity or injuries.
Therefore, when the language axis is functionally isolated from a particular source of information about which the patient is questioned , it begins to make up a response based on the information available, even if that information is completely irrelevant. However, if the language axis is flooded with information, it is unable to determine what is relevant and begins to express fantastical confabulations.
CONFABULATION DUE TO FRONTAL LOBE INJURY
When secondary to right (or bilateral) frontal damage, speech may become exceedingly bizarre, delusional, and fantastical, as loosely associated ideas become organized and anchored around fragments of current experience.
For example, when one frontal lobe patient was asked as to why he had been hospitalized, he denied that there was anything wrong with him, but instead claimed he was there to do some work. When asked what kind of work, he pointed to the air conditioning unit, and stated: "I'm a repair man. I'm here to fix the air conditioner. Now, if you'd please excuse me. I've got work to do."
A 24 year old store clerk who received a gunshot wound (during the course of a robbery) which resulted in destruction of the right inferior convexity and orbital areas, attributed his hospitalization to a plot by the government to steal his inventions (Joseph 1986a). He claimed he was a famous inventor, had earned millions of dollars and had even been on TV. When it was pointed out that he had undergone surgery for removal of bone fragments and the bullet, he pointed to his head and replied, "that's how they are stealing my ideas."
Another patient, formerly a janitor, who suffered a large right frontal subdural hematoma (which required evacuation) soon began claiming to be the owner of the business where he formerly worked (Joseph 1988a). He also alternatively claimed to be a congressman and fabulously wealthy. When asked about his work as a janitor he reported that as a congressman he had been working under cover for the C.I.A. Interestingly, this patient, also stated he realized what he was saying was probably not true. "And yet I feel it and believe it though I know it's not right."
Frontal lobe confabulation seems to be due to disinhibition, difficulties monitoring responses, withholding answers, utilizing external or internal cues to make corrections, accessing appropriate memories, maintaining a coherent line of reasoning, or suppressing the flow of tangential and circumstantial ideas (Fischer et al. 1995; Joseph 1986a,1988a, 1999a; Johnson, O'Connor and Cantor 1997; Kapur and Coughlan 1980; Shapiro et al.1981; Stuss et al. 1978; Stuss and Benson 1986). That is, since the right frontal lobe can no longer regulate information processing and the flow of perceptual and ideational activity, information that is normally filtered out and suppressed is instead expressed. In consequence, the Language Axis of the left hemisphere becomes overwhelmed and flooded by irrelevant, bizarre associations, leading sometimes to the expression of false memories, which the patient (that is, Broca's area) repeats (Joseph, 1982, 1986ab, 1988ab).
Frontal injuries, therefore, may result in the production of fantastical spontaneous confabulations where contradictory facts are ignored or simply incorporated into the patient's ungoing speech. This is because the language axis of the left hemisphere has become overwhelmed and flooded by irrelevant associations (Joseph, 1986a, 1988a, 1999a). In some cases the content of the confabulation may border on the bizarre and fantastical as loosely associated ideas become organized and anchored around fragments of current experience.
For example, one patient with a degenerative disturbance that involved predominantly the right frontal lobe, at times claimed to be a police officer, a doctor, or married to various members of the staff. When it was pointed out repeatedly that he was a patient, he at one point replied, "I'm a doctor. I'm here to protect people."
GAP-FILLING
Confabulation is also associated with lesions that involve the posterior, parietal lobe portions of the right hemisphere, immaturity or surgical section of the corpus callosum, or destruction of fiber tracts that lead to the left hemisphere (Joseph, 1982, 1986ab, 1988ab; Joseph et al. 1984). With damage to these brain areas, there is incomplete information transfer to and reception within the language axis.
As a consequence, because the language axis of the left hemisphere is unable to gain access to needed information, it attempts to fill the gap with information that is related in some manner to the fragments received. However, because the language areas are disconnected from the source of needed information, it cannot be informed that what it is saying (or, rather, making up) is erroneous, at least insofar as the damaged modality is concerned.
For example, in cases presented by Redlich and Dorsey (1945), individuals who were suffering from blindness or gross visual disturbances due to injuries in the visual cortex continued to claim that they could see even when they bumped into objects and tripped over furniture. Apparently, they maintained these claims because the areas of the brain that normally would alert them to their blindness (i.e. visual cortex) were no longer functioning.
CONFABULATION, NEGLECT, & DELUSIONAL DENIAL
Confabulation and delusional denial also often accompany neglect and body-image disturbances secondary to right cerebral (parietal) damage (Joseph 1982, 1986a, 1988a). For example, the left hemisphere may claim that a paralyzed left leg or arm is normal or that it belongs to someone other than the patient. This occurs in many cases because somesthetic body information no longer is being processed or transferred by the damaged right hemisphere; the body image and the memory of the left half of the body have been deleted. In all these instances, however, although the damage may be in the right hemisphere, it is the speaking half of the brain that confabulates.
According to Geschwind (1965), when the speech area is disconnected from a site of perception, then the speech area will be unable to describe what is going on at that site. This is because "the patient who speaks to you is not the 'patient' who is perceiving- they are in fact, separate".
In these instances delusions and confabulatory responses occur as a result of an attempt by the Language Axis to fill the gaps in the information received with associations and ideas which are in some manner related to the fragments available (Joseph, 1982, 1986a, Joseph et al. 1984; Talland, 1961). In this regard, confabulatory-delusional statements although erroneous, can contain some accurate elements around which erroneous, albeit related, ideations are anchored. Hence, a patient may see his left leg or arm and then state it belongs to the doctor. In general, these disturbances occur most frequently when the right frontal or right parietal lobe is damage. However, neglect, denial, and delusional confabulation may also infrequently result from left parietal injuries.
Nevertheless, not uncommonly, patients with right parietal lesions, when confronted with their unused or immobile limbs may (at least initially) deny that it belongs to them or swear there is nothing wrong (Gold et al. 1994; Heilman 1991; Joseph, 1986a, 1988a). More often, however, they tend to ignore their left half.
In some cases, however, patients with right parietal injuries may perceive and acknowledge the left half of their body but mah refer to it using ego-alien language, such as "my little sister", "my better half", "my friend Tommy" , "my brother-in-law", "spirits", etc.
For example, Gerstmann (1942) describes a patient with left-sided hemiplegia who "did not realized and on being questioned denied, that she was paralyzed on the left side of the body, did not recognize her left limbs as her own, ignored them as if they had not existed, and entertained confabulatory and delusional ideas in regard to her left extremities. She said another person was in bed with her, a little Negro girl, whose arm had slipped into the patient's sleeve" (p. 894). Another declared, (speaking of her left limbs), "That's an old man. He stays in bed all the time."
One such patient engaged in peculiar erotic behavior with his "absent" left limbs which he believed belonged to a woman. A patient described by Bisiach and Berti (1987, p. 185) "would become perplexed and silent whenever the conversation touch upon the left half of his body; even attempts to evoke memories of it were unsuccessful". Moreover, although "acknowledging that all people have a right and a left side, he could not apply the notion to himself. He would affirm that a woman was lying on his left side; he would utter witty remarks about this and sometimes caress his left arm".
Some patients may develop a dislike for their left limbs, try to throw them away, become agitated when they are referred to, entertain persecutory delusions regarding them, and even complain of of strange people sleeping in their beds due to their experience of bumping into their left limbs during the night (Bisiach & Berti, 1987; Critchley, 1953; Gerstmann, 1942). One patient complained that the person tried to push her out of the bed and then insisted that if it happened again she would sue the hospital. Another complained about "a hospital that makes people sleep together". A female patient expressed not only anger but concern least her husband should find out; she was convinced it was a man in her bed.
DISCONNECTION, GAP FILLING, & THE LANGUAGE AXIS
To be informed about the left leg or left arm, and to then make verbal statements about the left half of the body, the language axis must be able to communicate with the cortical area (i.e. the parietal lobe) which is responsible for perceiving and analyzing information regarding the extremities. When no message is received and when the language axis is not informed that no messages are being transmitted, the language zones instead relie on some other source even when that source provides erroneous input (Joseph, 1986a); substitute material is assimilated and expressed and corrections cannot be made (due to loss of input from the relevant knowledge source). The patient begins to confabulate.
Of curse, in some respects it seems quiet puzzling that individuals with right parietal injuries may deny what is visually apparent and what they should easily be able to remember, i.e. the presence of the left half of their body. However, it is possible that when the language dominant left hemisphere denies ownerhip of the left extremity it is in fact telling the truth. That is, the left arm belongs to the right hemisphere not the left hemisphere. Indeed, in that the parietal lobe maintains body image memories, destruction of the parietal lobe can erase those memories such that the patient, that is, the language axis, is unable to gain access to those memories and then denies ownership of the left half of the body.
This is because the left hemisphere maintains a somesthetic-memory image of only the right half of the body. The right cerebrum maintaining perhaps bilateral representations. In this regard, the left brain may in fact have no memory regarding the left half of the body.
CONFABULATION & SELF DECEPTION:
A Common Characteristic of the Human Condition.
Humans in general, often lack insight into the causes of their behavior and confabulate what they believe to be reasonable explanations for their actions. For example, in an experiment conducted by Nisbett and Wilson (1978), shoppers were asked to indicate their preferences and to choose among four stockings which in fact were completely identical. The majority of shopper picked the stocking to their right, even though the experimenters continually shifted the position of the stockings.
When asked why they picked "that particular stocking", all invented perfectly logical explanations: The color, shape, texture, and so on. However, the real reason was that most humans are right handed and display a right sided response bias. Since that information was not available to the language regions of the left half of the brain, it instead made up acceptable explanations.
Likewise, when it comes to sexuality, some women also make up acceptable explanations for their behavior: "he raped me!"
JENNIFER: A CASE STUDY IN SEXUAL SELF-DECEPTION
Jennifer has a conservative background and well meaning upper middle class, semi-religious parents, who impressed upon her the need to maintain certain values and morals. Jennifer is in her first semester at college and living in the dorm, and like all freshmen, she is required to attend a standard college lecture on sexual harassment, which essentially explains that a woman should feel offended and harassed if a man compliments her clothes or tries to kiss her after a date unless she expressively gives him permission, and that his behavior is inappropriate and unwelcome unless she tells him it is OK.
One day a handsome, muscular, sexy, upper clansman whom she has seen about campus, invites her out. She happily consents. They have dinner, stop at a local nightclub, dance close together and have a drink. So far it has been an exciting, romantic evening.
On the way back to the dorm he invites her to stop by his place to "check out the new CD player and stereo equipment" he had just purchased. She knows, or rather, is aware of the sexual nature of his intentions and what might happen if she stops by his place. Indeed, the look in his eyes, his tone of voice and body language had made his sexual interests completely clear to the right half of her brain and limbic system before they even began dinner.
Despite this awareness of his sexual intentions and what would likely take place once she arrives at his apartment, the left half of her brain refuses or is unable to acknowledge these sexual possibilities. Insofar as the left half of her brain is concerned this fine fellow just wants to show her his stereo.
As she does not want to or is unable to acknowledge this sexual awareness, the left half of her brain begins to invent and think up reasons why it is OK to go to his apartment. He seems real nice. They have had a real good time. He has not acted inappropriately. Why not?
Once at his home he makes certain advances; sitting close to her, looking in her eyes, he tells her she is "really beautiful." Her limbic system and the right half of her brain, responding to his body language, the inflection in his voice, etc., is certain of his sexual desires and what he means by his words. Moreover, she is not only aware of what might occur next, she is also aware that she may have to make a decision regarding this. However, she does not want to "think about that" (she is a nice girl).
Due to her conscious self-image this information and all sexual implications are suppressed and ignored. The language dominant left half of her brain does not gain access to what the right half of her brain and limbic system is fully aware of. The left hemisphere thinks: this guy is only being really nice.
He places his hand on her knee and caresses her skin. The act risks changing the situation by calling for an acknowledgment and an immediate decision as to its sexual meaning. To leave his hand there is to consent, to acquiesce to his sexual desires and to consciously acknowledge them willingly. Yet to withdraw his hand is not only a recognition of what it implies, but a refusal. Her aim is to postpone her decision, to stall conscious recognition. She has "no idea" as to what he is up to. She leaves his hand there because she "doesn't notice it."
And yet, as they talk, he has moved closer to her, his hand slowly gliding past her knee, slipping beneath her skirt, touching her silky thighs. But she is concentrating on what he is saying, the curve of his lips, the white of his teeth, her reply to his questions; this is what she is verbally conscious of. She reacts as a personality that does not know that a hand is fondling her leg. She is being seduced.
She is also being self-deceived. She has restricted the verbal aspects of consciousness and her verbal thoughts to only selective (verbal) aspects of what is occurring. She is failing to verbally acknowledge consciously what she is fully aware of emotionally and sexually. Indeed, she is (non-verbally) aware that his actions are sexual and she has been aware of everything that might occur since the moment he asked her out--which is why she consented to go out with him!
However, if someone were to have told her this fellow would bring her home and make possible sexual advances, she would have turned down the date. After all, her conscious self-image is that of a "good girl," a "nice girl." As she has always told her friends, she will have sex only with a man that she loves. The "thought" of "sex" was so far from her (conscious) mind that she never, never "thought" he would make sexual advances.
So why did she go out with him? Why is she not taking his hand and indicating that his behavior is not acceptable: "Please stop." One would have to assume that her limbic system was "turned on," she was sexually attracted to him, and the possibility of his making sexual advances was not only acceptable but welcome; at least on an unconscious, limbic level.
Yet, what is acceptable to her limbic system is not acceptable to the linguistic aspects of consciousness and her conscious self-image. Unconsciously, at the level of her limbic system, although she is in fact sexually yielding to his and her desires, from the perspective of the linguistic aspects of her conscious mind, she still does not know what is going on. His behavior seems harmless.
There is a possible unity in a situation such as this, for her actions necessitate a recognition of the sexual intentions of her male friend as well as a disavowal (Sartre, 1956). Otherwise she would have asked: "What is your hand doing on my thigh? Why are you pulling down my panties? Please stop!!!"
Even if unable to verbalize her conscious disapproval (as some young women become too intimidated to speak up) she would have made some attempt to back off or disengage herself if sex is not what she wanted. Consciously and verbally, she is disconnected from sexual reality--that is, if she claims innocence--a sexual reality that she is sexually aware of. So she seemingly does nothing but in fact is completely acquiescing and encouraging his sexual behavior.
This is the beauty of self-deception and the organization of the mind and brain, it allows a person to engage in a certain behavior while simultaneously avoiding responsibility for that behavior and enabling them to preserve their conscious self-image. It preserves the possibility of an event occurring or a desire being acted upon while believing that the event or action is not occurring. It enables an individual to completely avoid responsibility for their behavior.
In Jennifer's case, the language axis of her brain is disconnected from those sexual impulses arising in the limbic system and the right half of her brain, and/or has chosen to mislabel these impulses, calling them what they are not (Joseph, 1982). In this regard it could be said that the left half of her brain is unconscious, or rather, not conscious of these sexual impulses; an inter-psychic arrangement which allows her to deceive herself into thinking she is not responsible for her own sexual behavior or for what happens next.
He leans close and kisses her upon the lips as he runs his hand along her inner thigh, and plays at her panties. The kiss takes her by "surprise." He snakes his other arm around her and kisses her again as the fingers of his other hand slips beneath her panties.
She is breathing hard, kissing him, feeling his probing fingers... she does not know what to do. She is confused yet excited. Her limbic system is proclaiming: "I want it now!" and her right hemisphere is also a willing participant.
It is the language depending aspects of consciousness, and those aspects of mental activity depending on words for thinking, which are completely disconnected, which does not know what is going on or why. Verbally, the language axis of the left half of her brain may be completely ignorant as to what is taking place and in all innocence is saying: "What's going on?"
He continues kissing her and with his fingers is touching her passionately. She feels herself yielding as her limbic system begins to overwhelm her conscious inhibitions, hijacking the neocortex and the language depending conscious mind. He is touching and probing her with his fingers, while with his other hand he slips his hand and fingers beneath her bra. Jennifer moans and feels as if she is about to swoon.
Her limbic system, in effect, has taken over, and the frontal lobes and neocortex have essentially gone "off line." From a verbal, rational perspective, she is now a passive observer to behavior over which she, i.e., her neocortex has no control; for it is the limbic system which governs sexual behavior.
He kisses and probes her passionately and expertly removes her blouse, and then her bra... and later... her panties... and spreading her legs, his fingers deep inside, he lights a fire of yearning desire, and then ever so gently, he enters her making her moan and gasp and then beg, beg, "Oh...Baby!!! Oh...Baby!!!" for more.
Unfortunately for the two love birds: Later, when Jennifer's limbic system was completely satiated and no longer sexually aroused, and as her neocortex and left hemisphere regained control, she began to feel guilty and was then shocked at what the rest of the brain had done... What he had done! For certainly her left hemisphere was not a willing participate. That's it! Since it was unwilling, then she must have been tricked...or forced to have sex. He forced her! He took advantage of her. He... He... He raped her! She may even convince herself that she is "still a virgin."
Indeed, it often happens that people behave in a certain manner, or say certain things that are shocking even to themselves. They don't know "what came over" them. They may see themselves as moral, just, kind, loving, and for some unknown reason act in a cruel, selfish, sexual or spontaneous manner and yet retain the conviction that what they have done or said is not a true representation of how they really feel or who they really are. Often, however, once the limbic system has been satisfied and the neocortex, frontal lobes, and language axis regains dominance, it may then begin to think guilty thoughts and impose feelings of guilt on itself.
The object is to avoid these feelings of guilt. To avoid responsibility for one's behavior. Hence, since Jennifer was (in her opinion) obviously "taken advantaged of" by "that rat," "that scoundrel," "that womanizer," "that pig," then she is of course not responsible for what happened. She "had no idea as to what he was up to," or that "he was that kind of guy" and that he would pull off her panties and "rape" her. And, besides she "had too much to drink," (although she in fact had only one) and "was too tired to fight him off," (although she never tried) and before she "knew it, it was too late," and so on. Her conscious, verbal, self-image remains untarnished. She is free of conscious guilt. She has deceived herself.
And yet, she knows and is aware of the truth. It is precisely because she knows that she feels compelled to engage in self-deception and invent innumerable excuses for her behavior; deceptions other females may accept if they have also been indoctrinated into believing that women are victims of male sexual predators and that women are not always responsible for their sexual behavior.
However, let us be clear, self-deception has no sexual orientation. Among men, peoples, races, and nations, confabulation and self-deception is an accepted and necessary aspect of the human condition--a function of language and the functional organization of the human brain.
REFERENCES






