





by Rhawn Joseph, Ph.D.
Rhawn Joseph, Ph.D.
BrainMind.com
Dyslexia is a disturbances in the ability to read, whereas alexia refers to a complete loss of reading ability. In general, whereas dyslexia is primarily a congenital disturbance, alexia is an acquired disorder and is due to a neurological injury generally in the vicinity of the temporal, occipital, parietal lobe. ALEXIA
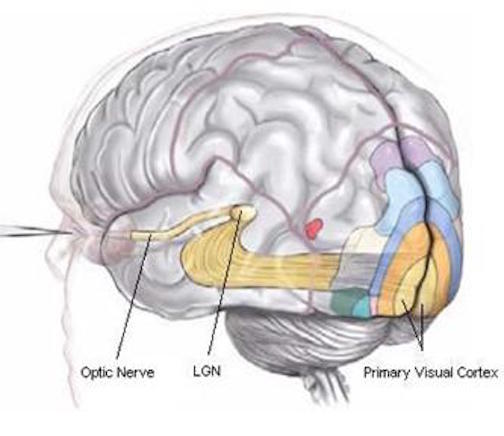
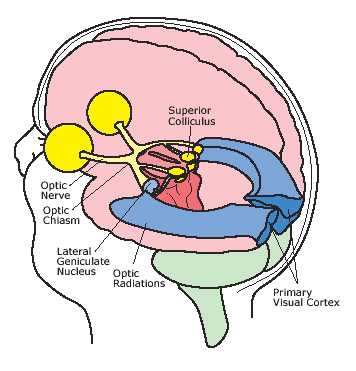
There are a variety of theories which purport to explain the mechanisms involved in reading and the comprehension of written language. Reading, of course, requires activation of the visual areas in the occipital and temporal lobes, so that the symbolic form of the letter or word is perceived, which in turn enables the viewer to determine that the form is a letter or a series of letters making up a word.
However, not only must letters or groups of letters be recognized and their temporal order ascertained (referred to as "orthographic" processing); but there must be semantic processing. That is, the letters and words are perceived and then the relation of a series of letters or words to each other are recognized so that the meaning of the word or sentence can be derived.
Words are not only seen and thus read, but the sound of the written word, as it is read (or written) may "be heard" within the privacy of one's head. This is referred to as the "phonological" aspect of reading.
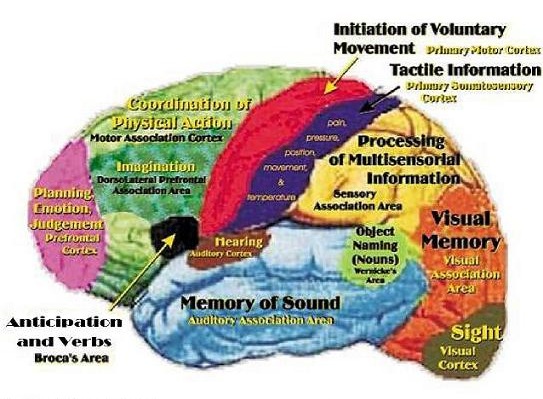
The phonological stages of reading and linguistic analysis involves activation of Wernicke's receptive speech area (in the temporal lobe) and Broca's expressive speech area (in the frontal lobe). In some cases, individuals will move their lips as they read, which is due to activation and participation of Broca's area which programs the oral musculature for the purposes of speech.
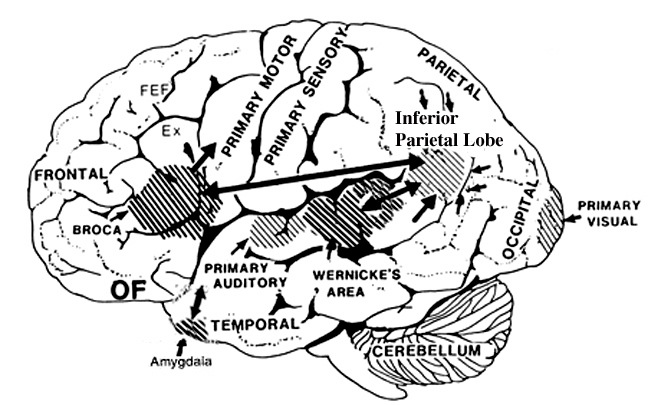
Yet another region of the brain that contributes significantly to reading ability is the inferior parietal lobe (IPL). The IPL becomes highly active when reading, as demonstrated by functional imaging (Demonet, et al., 2004; Paulesu, et al., 2013; Price, 2007).
Different regions of the brain, therefore, interact during various stages of reading, such that in consequence, abnormalities of or lesions to different areas can result in different types of reading abnormalities.
For example, a small lesion to one area of the brain, may result in an inability to recognize sentences or long words, whereas the ability to recognize letters and short words remains intact. With damage to yet another brain area, the patient may suffer fraom an inability to derive semantic meaning from words once they are read.
In some cases,the patient may lose the ability to read, but retains the ability to write, and can spell and write the very words he cannot read. (Coltheart, 1998; Miceli et al., 2009; Miozzo & Caramazza, 1998; Goodglass & Kaplan, 2000).
For example, injuries the left IPL can disrupt the ability to read and spell. This is because the IPL matches auditory images to visual images and associates both so as to form multimodal concepts including those necessary for reading and the comprehension of written language. However, this disorder is due not only to IPL damage, but to disconnection from the occipital and temporal lobes which perform visual and auditory functions.
Damage to the IPL or to the superior temporal lobe, can also disrupt the ability to spell by sound and to engage in phonological processing, such that patients can no longer hear (in their head) the sound of the words they are reading, nor can they match the sounds they hear to the visual-motor components of reading (the generation and comprehension of visual symbols, i.e. words and letters).
The Loss of the ability to engage in phonological processing or to spell by sound is a common feature of dyslexia and alexia (Brady & Shankweiler, 2011; Miceli et al., 2009) and is common with middle temporal lobe injuries.
Injuries to Wernicke's area (and thus the left superior temporal lobe) also disrupts reading, writing, and all aspects of linguistic comprehension. Not only is reading compromised but patients may lose the ability to comprehend spoken language.
Individuals diagnosed as suffering from developmental dyslexia have frequently been found to have abnormalities in temporal lobe and IPL , 2007) as well as in the IPL and left superior temporal lobe (Denays et al., 1989; Galaburda et al., 2005); Rumsey et al., 1992; Tzourio et al.,2004). The IPL and the temporal lobe thus appear to be the primary structures involved in reading.
The IPL, middle temporal lobe, and Wernicke's area are richly interconnected, and in some respects coextensive. These areas are also linked to Broca's Expressive speech area and the frontal motor areas, which is why some people move their lips when they read.
THE NEUROLOGY OF READING.
From a neurodynamic perspective the process of reading involves the perception and analysis of visual impulses in the primary and association visual receiving areas (in the occipital lobes). This information is next transferred to the visual association cortex where higher level information processing is carried out and visual associations formed. These visual associations are next transmitted to a variety of areas (Haxby, et al., 2011; Peterson, et al., 1988, 1990; Price, 2007; Zeki, 2007) including Broca's and Wernicke's area, the inferior and middle temporal lobe and the IPL. It is in these latter cortical regions where multimodal and linguistic assimilation take place so that the auditory equivalent of the visual stimulus may be retrieved. That is, via these interactions visual grapheme clusters become translated into phonological sound images. In this manner we know what a written word looks and sounds like. It is also possible, however, to bypass this phonological transcoding phase so that word meanings can be directly accessed (i.e. lexical reading).
THE DEVELOPMENT OF READING. It is generally believed, in learning to read, that visual symbols are recognized as graphemes (letters) and that these graphemes are decoded and then converted to phonemes (via the IPL which performs an auditory matching function), i.e. phonological analysis. In this manner, the child learns to associate written symbols with spoken words.
This requires that written (and verbal) language also be broken down into syllables and phonemes so that auditory-visual associations can be made; i.e. "phonological awareness." The sound of the word is matched with its visual image.
The greater a child's phonological awareness, the greater is their reading ability (Brady & Shankweiler, 2011).
Presumably, it is only after the child develops their phonological awareness, and after increased experience with reading, that they are able to bypass the phonological transcoding phase and engage in lexical reading. Thus, as the childs ages and learns to read, phonological processing becomes subsumed and employed only secondarily when confronted with unfamiliar words.
THE NEUROLOGY OF READING
Although it is likely that most individuals utilize both lexical and phonological strategies when reading, in either case the temporal-parietal-occipital lobes are all implicated. These structures all participate, to varying degrees in phonological and lexical processing. Indeed, as demonstrated through functional imaging, reading activates Wernicke's area and the left posterior temporal lobe (Bookheimer, et al., 1995; Howard et al., 199), including the supramarginal gyrus (Bookheimer, et al., 1995), and angular gyrus (Price, 2007), the latter structures comprising the inferior parietal lobe. Conversely lesions to these different areas produce alexic disturbances.
SUBTYPES OF ALEXIA AND DYSLEXIA DEPEND ON LESION SITE
With lesions of the angular gyrus, or when damage occurs between the fiber pathways linking the left inferior parietal lobule with the visual cortex (i.e. disconnection), patients may suffer from Pure Word Blindness--also referred to as Pure Alexia (Coltheart 1998; Miozzo & Caramazza, 1998). Patients can see without difficulty, but are unable to recognize written language. Written words evoke no meaning.
However, because the left posterior basal temporal lobe is a convergence zone for visual, auditory, and tactile information, and becomes activated during a variety of language tasks, including reading and object and letter naming (Buchel et al., 1998; Price, 2007), if injured, patients may suffer from reading and naming deficits (Rapcsak, et al., 1987); a condition referred to as phonological alexia. Moreover, patients with developmental dyslexia have been found to have abnormalities in this latter area (Rumsey et al., 2007).
Thus there are several subtypes of reading disturbances which may occur with left cerebral damage or congenital disturbances involving these tissues (Coltheart 1998; Miceli et al., 2009; Miozzo & Caramazza, 1998). These include literal, verbal, and global alexia, and alexia for sentences, as well as developmental dyslexia. In addition, alexia can sometimes result from right hemisphere lesions, a condition referred to as Spatial Alexia. All these disorders, however, are acquired and should be distinguished from developmental dyslexia which is present since childhood (see Njiokiktjien, 1988).
DEVELOPMENTAL DYSLEXIA
Developmental dyslexia is one of the most common of all learning disabilities, effecting up to 8% of the school aged population. There is an obvious genetic foundation to this disorder, as is evident from the high familial risk rates that range from 35% to 45% (Smith et al., 1990) and many of these children suffered from even more profound language disorders during their preschool years, e.g. developmental dysphasia. Developmental dysphasias affect from 8% to 15% of all preschool children and most of these children, even as they acquire language, continue to suffer severe disturbances in reading and spelling (Aram et al. 1984); a function, in part, of not only brain abnormalities, but persisting deficits in phonological processing.
Congenital disturbances involving these tissues (dysplasia, ectopias), including the middle temporal lobes, the perisylvian regions and the planum temporal, are associated with developmental dyslexia (Galaburda et al., 2005). Using functional imaging, Rumsey et al. (1992) and Tzourio et al., (2004) found that dyslexic children failed to activate the left temporal-parietal cortex when engaged in word tasks, whereas Denays et al. (1989) found hypoperfusion in this same area.
PURE WORD BLINDESS. ALEXIA WITHOUT AGRAPHA
Pure alexia, or alexia without agraphia (due to the preservation of the ability to write) is a condition where patients are unable to read written words, or even recognize single letters (Coltheart 1998; Miozzo & Caramazza, 1998). However, if words are spelled out loud, they have little difficulty with comprehension (due to intact pathways from Wernicke's to the angular gyrus). Moreover, they are able to speak, spell as well as write without difficulty. Nevertheless, although able to write, they are unable to read what they have written.
In general, the lesion appears to be between the left angular gyrus and the occipital lobe (in the arterial distribution of the left posterior cerebral artery), and extends to within the splenium of the corpus callosum (Benson, 1979; Vignolo, 1983) which prevents right hemisphere visual input from being transferred to the inferior parietal lobe of the left half of the brain. Sometimes this condition is due to a tumor or following a head injury accompanied by a hemotoma involving the white matter underlying the inferior parietal lobule (Greenblatt, 1983) and or the temporal-parietal cortex (Rumsey et al. 1992). In these instances the left angular gyrus is unable to receive visual input from the left and right visual cortex and visual input cannot be linguistically translated. The patient cannot gain access to the auditory equivalent of a written word.
Although unable to read written language, this syndrome is not always accompanied by a visual field defect (hemianopsia). Moreover, objects may be named correctly (Hecaen & Kremimin, 1977). However, patients may suffer from color agnosia (Benson & Geschwind, 1969), i.e. an inability to correctly name colors. There is often (but not always) an inability to copy written material (because of disconnection from the visual areas) and many patients have difficulty performing math problems. In some cases the patient suffers not only pure word blindness but blindness for numbers as well.
This condition has been described as Global Alexia by some authors. However, global alexia is a more pervasive disorder in which the ability to write (agraphia) and name objects is also compromised.
ALEXIA FOR SENTENCES
Patients suffering from alexia for sentences are able to read letters and single words but are unable to comprehend sentences. However, patients may have difficulty with unfamiliar or particularly long words whereas more familiar material is easily understood. Lesions are usually localized within the dominant occipital lobe but may extend into the inferior parietal area.
VERBAL ALEXIA
When patienta are able to read and recognize letters but are unable to comprehend or recognize whole words they are said to be suffering from verbal alexia. However, if presented with short words their reading ability improves. Hence, the longer the word the greater the difficulty reading (Hecaen & Albert, 1978). Verbal alexia usually results from lesion involving the dominant medial occipital lobe (Hecaen & ALbert, 1978; Hecaen & Kremin, 1977).
LITERAL/FRONTAL ALEXIA
When the patient is unable to recognize or read letters this is referred to as Pure Letter Blindness. Patients are usually unable to read by spelling a word out loud, and the abilty to read numbers and even musical notion is often disturbed. Some authors have attributed literal alexia to left inferior occipital lesions (Hecaen & Kremin, 1977).
This disorder has also been referred to as Frontal Alexia. This is because individuals with Broca's aphasia or lesions involving the left frontal convexity have difficulty reading aloud, and have the most difficulty with single letters rather than whole words (Benson, 1977).
SPATIAL ALEXIA
Spatial alexia is associated predominantly with right hemisphere lesions. In part this disorder is due to visual-spatial abnormalities including neglect and inattention. That is, with right cerebral lesions the patient may fail to read the left half of words or sentences, and may in fact fail to perceive or respond to the entire left half of a written page.
Right posterior injuries may also give rise to spatial disorientation such that the patient is unable to properly visually track and keep place, their eyes darting half hazardly across the page. For example, they may skip to the wrong line. Spatial alexia may also result from left cerebral injuries in which case it is the right half of letters, words and sentences which are ignored (Marshall & Newcomb, 1973). Indeed, patients not only ignore words, but sometimes the left half of the bodies and the entire left half of visual space. Hence if they are presented with the words "help me"they may only see help. Of if they read: "toothbrush" they may only see the word "tooth." However, if they were presented only with the word "tooth" they would see only "too." This latter form of spatial alexia is thus really a subtype of generalized left sided neglect and is common with right cerebral injuries.










