





Rhawn Joseph, Ph.D.
W. Haven V.A. Medical Center, Yale University Seizure Unit,
UHS/The Chicago Medical School, Chicago, USA
ABSTRACT
A Case study of a "split-brain" right-handed individual with epilepsy and brain dysfunction of early onset is described who was found, following callostomy (sparing the rostrum of the callosum) to be left hemisphere "dominant" for processing and/or expressing emotional and somesthetic information ,and right hemisphere "dominant" in regard to the expression and comprehension of language and linguistic stimuli. Hence, a significant reversal in functional representation, due presumably to an injury suffered early in life, was observed. Moreover, following callosotomy the patient demonstrated severe disconnection syndromes in regard to right hand usage, the recognition of emotion, and the production and comprehension of linguistically related information. The left cerebrum appeared to be almost completely without linguistic representation except in regard to emotional language. The possible mechanisms involved in functional sparing and reversed representation are briefly discussed, and the effects of partial disconnection on the expression of these capacities is presented.
INTRODUCTION
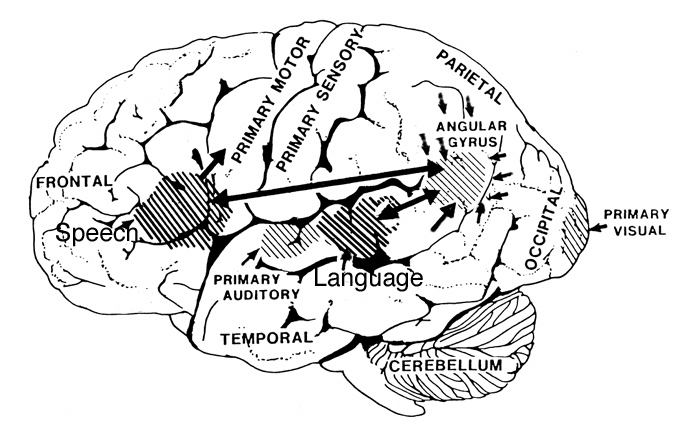
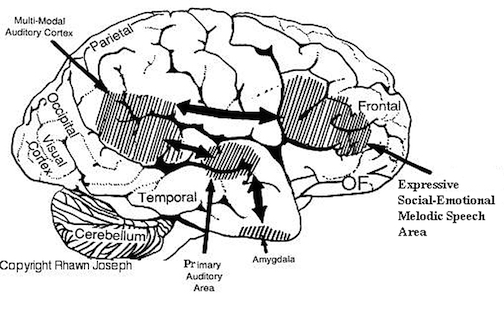
Approximately 89% of the population are genotypic right handers, of which 90-96% have been estimated to be left hemisphere dominant for expressive and receptive linguistic functions and fine motor control. In contrast, the right cerebral hemisphere has been associated with the mediation of visual-spatial, tactile, and emotional information processing, as well as the expression and comprehension of prosodic (intonation, melody) and emotional language.
However, because the right cerebrum matures later, when the brain is damaged early in life (as in birth trauma), the left cerebrum is often more seriously affected such that handedness and language may secondarily come to be subserved by the right. However, in some instances early left hemisphere lesions may instead result in atypical left hemisphere language localization.
Secondary acquisition of language by the right hemisphere appears to occur at the expense of certain right hemisphere capacities (for example visual-spatial), such that these abilities are reduced. It has been suggested that these functions are sacrificed because capabilities normally subserved by the left competitively "crowd" out later appearing functions mediated by the right; that is, by growing into "vacant" synaptic space. In primates, early structural reorganization resulting from competitive acquisition of functionally "vacant" synaptic space has been well demonstrated. In instances, such as these the functions that are displaced via crowding are grossly diminished as structural space is presumably committed.
Nevertheless, it remains possible, in cases where language has migrated owing to early left cerebral injury, that right hemisphere capacities may come to be secondarily subserved by "vacant" undamaged areas in the left which are no longer committed to language representation. As such, a partial reversal in functional dominance is a strong possibility.
In the following case, a right-handed individual with a brain injury and dysfunction of early onset was found to be right hemisphere dominant for language (as determined via dichotic listening and sodium amytal studies). Within two weeks of callosotomy (performed to control intractable seizures) it was determined that his left hemisphere was "dominant" for processing and/or expressing emotional and tactile information but had little or no capacity for performing expressive language related tasks. For example, although formerly strongly right hand dominant in regard to most forms of motor activity including writing, following callosotomy he was able to use this hand for writing only with great difficulty. In contrast, when requested to write with the left hand he at first refused stating that it was "impossible" but with considerable surprise discovered that he could indeed write with ease.

History and Preoperative Evaluation
PC (partial callosotomy), a 20-year-old right hand dominant Caucasian male, was a product of a term pregnancy with a difficult high forceps delivery and began having epileptic seizures at age 8 years characterized by staring, unresponsiveness, drooling, and picking at this clothes. These would last seconds to minutes with 15-30 minutes post-ictal confusion. PC experienced 9-15 seizures per month.
Preoperative examination indicated that PC performed best with his right hand across all motor-related tasks whereas he employed the left with difficulty. Perceptual-spatial organizational and related skills were found to be moderately impaired. Expressive speech and receptive language functioning was within normal limits. Employing the WAIS as a measure of conceptual functioning, PC obtained a Verbal IQ of 94, a Performance-perceptual IQ of 86, and a Full Scale IQ of 90 which placed him in the average range overall at the 25% rank.
Baseline EEG showed moderate left hemisphere slowing with moderate to marked posterior slowing bilaterally. Irregular high amplitude sharp beta and delta activity was noted in the anterior regions bilaterally and in the right posterior cortex with spike and waves in the left frontal-temporal area. Depth electrode EEG monitoring on 16 channels revealed three independent spike foci. However, CT scan appeared normal. Since it was believed that the seizures were spreading between the cerebral hemispheres via the corpus callosum, callosotomy with sparing of the rostrum and anterior commisures was performed (by Dr Dennis Spencer of the Yale University Dept of Surgery).
Prior to surgery assessment of hemisphere specialization for receptive linguistic functioning was assessed and also determined via dichotic listening (see Methods and Results). Vocabulary, word knowledge, verbal abstract reasoning, and verbal judgment were determined to be within average (normal) limits. A significant left ear dominance for dichotically presented verbal stimuli was also established. This dominance markedly increased following callosotomy. Intracarotid sodium amytal ("Wada test") injections confirmed right hemisphere dominance for speech. No expressive abilities were demonstrated following the right hemisphere injection, indicating that the left hemisphere of this patient was unable to talk. Hence, right hemisphere dominance for both receptive and expressive language was indicated.
Immediately following surgery the patient was mute and unable to express himself linguistically. This condition rapidly cleared over the next several days. When evaluated 2 weeks later, PC complained of decreased sensation in the left extremities (which was confirmed via neurological and neuropsychological evaluation), and decreased motor control over the right extremities. In contrast, sensation was adequately appreciated when applied to the right side and he had no difficulty with left sided motor control. The Boston Diagnostic Aphasia battery was administered and normal functioning determined. Nevertheless, the patient complained of a disturbance in his ability to write or making his formerly dominant right hand "do what I want it to." Attempts at writing were characterized by frequent erasures, hesitations, the production and crossing out of incorrect letters, misspellings, etc: "I know what letters I want, but I can't make my (right) hand write them." When asked to use his left hand PC at first declined protesting he could not. It was (to his great surprise) the discovery that he could use the left without difficulty, whereas when presented with emotional words the right hand suddenly regained its capacity to write and spell correctly, which led to the present investigation.
It is important to emphasize that conceptual, intellectual, and linguistic functioning was determined (pre-operatively) to be within average limits. The patient was literate, without dysphasic disturbances, and of normal personality.
Methods and Results
Emotional and Neutral Words:
PC was asked to write 10 orally presented neutral and 10 emotional words (for example 'shit') with the left or right hand, and each hand was timed for seconds to complete each word. The same words were presented for the left and right hand, although presentation was balanced with approximately a 10 minute delay for identical words.
As determined by seconds to completion, the right hand required an average of 11.8 seconds (5 preoperatively) and the left hand 6.8 seconds (15.5 preoperatively) to write each neutral word. This asymmetry was reversed when presented with emotional words, the right hand averaging 5.2 and the left hand 8.3 seconds. An analysis of variance (ANOVA) indicates that this interaction is significant, F(1, 36)= 12.2024, p< 0.01. Hence, the left hand was able to write emotional and neutral words at about the same time (p=NS), whereas the right hand performance improved and was superior to that of the left in response to emotional words.
Emotional vs Abstract vs Concrete Words
To investigate further the above mentioned asymmetries, words balanced for length and frequency of occurrence as determined by the Thorndike-Lorge word count were administered. PC was presented with 24 4-letter words (8-emotional, 8-concrete, 8-abstract) such that each hand wrote 12 different words (four from each category).
PC's right hand was clearly superior to that of the left hand for emotional words only (5 vs 9 seconds averaged for the right and left respectively). The left hand also took longer to write emotional (9seconds) as compared to concrete (5.5) or abstract (6.5) words. Conversely, PC's right hand took almost twice as long to write concrete (9.2) and abstract (11.9) vs emotional words (5), and as compared to the time taken by the left hand to write similar non-emotional material.
An ANOVA utilizing planned comparison was performed examining right vs left hand performance across these three variables. Significant effects for the right hand (simple comparison) were indicated, F(1,18)=6.144, p<0.05, such that abstract and concrete words were written more slowly than emotional words. Likewise, the right hand wrote emotional words more quickly than the left, F(2, 18)= 21.37, p<0.01. Hence, the right hand was more efficient with emotional stimuli, and the left hand performed in a superior manner when writing abstract and concrete words.
Blind Writing.
PC was blindfolded and given 10 trials in which he was asked to write orally presented neutral words with his right or left hand. Once blindfolded PC's ability to form letters and correctly spell words with the right hand (regardless of time allowed) was almost completely abolished. Over 80% of the right hand responses were characterized by misspellings (for example "tauple" for "table"). When using the left hand there was only a single error of omission as he failed to place 'r"'after the word 'chair.'
A Chi square analysis was performed and these differences were found to be highly significant (x2= 9.9, df=1, p<0.01).
Hence, when prevented from using visual cues PC's limited capacity to utilize the formerly dominant right hand for linguistic task is greatly diminished which in turn suggests (as evident by his frequent erasures, hesitations, etc. when allowed visual cues), that this limited capacity is actually secondary to cues transmitted from the right hemisphere and somehow direct his right hand performance.
Response to tachistoscopic visual stimuli Following the procedures and rationale outlined in detail elsewhere PC's right and left cerebral hemisphere were separately and individually presented with visual stimuli (that is 40 visual-pictorial scenes: for example, boy with a ball; 20 words: "hat"; and 10 numerals). All stimuli were presented 3 to the left or right of visual midline for 150ms. Visual field presentation order was counter-balanced and each stimulus was presented only once with the exception of the numerals (0-9) which were presented twice. Hence, each hemisphere was presented with 40 stimuli each (split-half design). Following right or left visual field presentation PC was asked to describe (and later point) to what he saw.
PC responded with 100% accuracy when the left visual field (right cerebral hemisphere) was presented with words or digits. In contrast, PC failed to identify any of the numbers presented to the right visual field and responded correctly to only two of the 10 words. A Chi square indicates that these differences are highly significant (x2= 13.33, df=1, p<0.001).
PC was later presented with the same stimuli to the right visual field and given a choice of four words (only one of which had been presented) in full field from which he was requested to "guess" the correct word via pointing (right hand). Of the 20 words presented PC 'guessed' correctly on only five items (25% accuracy which is less than chance).
When presented with numbers the results were similar (x2=20, df=1, p<0.001) such that left visual field performance was clearly superior to that of the right. Exactly the same results were found when eh was presented with visual-pictorial stimuli (x2=17.29, df=1, p<0.001) such that right visual field performance was clearly inferior to that of the left.
When presented with pictorial stimuli PC responded correctly to over 90% of the stimuli presented to the left visual field. In contrast, when stimuli were presented to the right visual field over 70% of his responses were contaminated by extraneous extrapolations, erroneous embellishments, and confabulatory ideation. For example, when stimuli were projected to the left visual field the right hemisphere responses were sparse and exact. In contrast, when a stimulus (for example, two boys fighting) was presented to the right visual field PC would respond "a boy. He is kneeling down and praying." Hence, although in some respects a correct element from the originally presented stimulus might be reported, much detail was deleted only to be replaced (that is the gap was filled) by erroneous ideation which at best was only tangentially related. This pattern of gap filling and confabulation following left hemisphere presentation is a reversal of that found with normal subjects as well as callosotomised adults. For example, in children, confabulation occurs largely only following right hemisphere stimulation, the language dominant left cerebral apparently "filling in" information incompletely received following inter-hemispheric information transfer.
When treated as a binomial (that is correct vs incorrect) these results are highly significant (p<0.05) and further indicate reversed asymmetry insofar as linguistic competence and functioning is concerned.
Recognition of Emotional Speech
Neutral phrases (for example "fish jump out of the water") were presented (via tape) in either a neutral, angry, happy, or sad tone, and PC was required to point with either the left or right hand to a face depicting one of these four emotions. Under each face (each of which "expressed" one of these emotions) was the corresponding word: happy, sad, etc. Thirty-two trials were administered. PC's right hand pointed to the correct face on all trials whereas 12.5% of the left hand responses were incorrect. A Chi square analysis indicates that these results are significant (x2=4.27, df=1, p<0.05).
Dichotic Listening
PC was presented dichotically with 120 trials consisting of words and 15 trials consisting of digits. PC failed to correctly identify any of the 15 digits presented to the right ear but correctly identified 14 of the 15 presented to the left ear (x2=26.25, df=1, p<0.001). Similarly, PC responded with almost complete suppression in regard to right ear word presentation, but correctly identified over 86% of the words presented to the left ear. Chi square indicates that these differences are also significant (x2=183.53, df=1, p<0.001).
Tactile Localization
While blindfolded a single finger on either the right or left hand was stimulated and PC was required to indicate the finger touched (using the thumb) either on the ipsilateral-stimulated (non-transfer) hand, or by using the thumb and fingers of the contralateral-nonstimulated (transfer condition) hand. As indicated in table 1, PC demonstrated little pre-operative difficulty with this task regardless of condition (transfer vs non-transfer). After operation, PC performed at 100% on the non-transfer trials. However, when required to indicate the corresponding finger on the opposite hand, 56% of the left to right hand transfer responses were in error, whereas 75% of the right to left sided transfer were erroneous.
These results are significant such that the right hand (x2=12.52, df=1, p<0.001) and left hand (x2=19.2, df=1, p<0.001) make more errors when transfer is required. From a comparison of the means, these findings suggest that PC has some difficulty when transfer is required and that the right hemisphere is less able to correctly respond when somesthetic stimuli are transmitted to it from the left cerebrum.
Temporal Sequencing
Using the procedure described above, a series of two or three fingers were successively stimulated on a single hand and PC was required to duplicate the pattern (using the thumb) either on the same (non-transfer) or contralateral (transfer) hand. This task, 120 trials, was administered both before and after operation.
As depicted in the table, preoperatively PC performed 100% of the transfer trials correctly, with a single error for each hand on the ipsilateral trials. Post-operatively, 25% of the left hand non-transfer trials were incorrect, whereas 80% of the right sided responses were erroneous. These differences are highly significant such that the right hand makes significantly more errors on non-transfer trials than does the left (x2=12.13, df=1, p<0.001).
When transfer of sequence is required, 85% of the responses were incorrect regardless of transfer direction (right to left, left to right). These results suggest that PC's left hemisphere has considerable difficulty performing operations involving temporal sequencing, a capacity, in part, greatly related to linguistic competence. Given the superior performance of the left cerebrum on the tactile localization task these errors are not likely to be secondary to deficits in localization or somesthesis. This view is further substantiated by the superior performance of the left hand on the sequencing task but the relatively inferior performance on the localization task.
Double Differential Simultaneous Tactile Stimulation
This task and procedures (described in detail elsewhere) involved simultaneously stimulating both hands (while out of view) with either the same or two different types of textured material (for example sandpaper, velvet; one to each hand) and then requiring PC to identify the stimuli by pointing to sample textures which were in view. Tactile suppressions were scored when PC failed to note and identify the stimulus applied to either left or right hand. He was assessed both pre- and post-operatively.
Prior to surgery, PC demonstrated a tendency to suppress with either the left or right hand (equally) on 27% of the trials. Post-operatively, PC demonstrated right hand suppression on 36% of the trials (x2= 1.53, df=1, p=NS, pre-vs post-operative results), and left hand suppressions on 60% of the trials (x2= 17.05, df=1, p<0.001, pre-vs post-operative performance). Left vs right hand performance (post-operative) did not significantly differ although the means are certainly suggestive of qualitative differences. Hence, these findings further suggest that the left hemisphere of PC has a superior capacity for perceiving, localizing, and identifying somesthetic stimuli.
Tactual-Object Matching
For this task, PC was required to point to various geometric shapes which corresponded to shapes tactually explored while out of view. PC was given both transfer (for example tactual exploration with the right hand, pointing with the left) and non-transfer trials utilizing a circle, square, triangle, and cross (task referred to as: Tactual-Visual Matching). In addition, similar to the procedures employed above, PC was also assessed in regard to his ability to tactually recognize shapes which were not in view. Hence, once a shape was tactually explored, he was required to release it and then individually explore similar shapes (differing in size and thickness) until he discovered the original (refer to as Tactual-Tactual matching).
When required to palpate and visually match a geometric shape (Tactual-Visual matching) with the right hand, errorless non-transfer (ipsilateral) and transfer (right to left hand) performance was observed. In contrast, 37.5% of the left hand (non-transfer) ipsilateral trials were erroneous. Hence, when the hands are compared the non-transfer performance of the left hand is clearly inferior to that of the right (x2=7.39, df=1, p<0.01). Moreover, when transfer is required the performance of the left hand deteriorates further such that significantly more errors are committed when transfer vs non-transfer performance is required (x2=7.39, df=1, p<0.01).
On the Tactual-Tactual matching tasks, right hand performance on the non-transfer trials was without error, whereas 50% of the left hand responses were incorrect. These right vs left hand performance differences are significant (x2=10.67, df=1, p<0.01). Moreover, transfer from the right to left hand resulted in a 25% error rate (right hand transfer vs non-transfer: x2= 4.57, df=1, p<0.05) whereas 50% of the left to right hand transfer responses were erroneous. Hence, when somesthetic information processing involves PC's right hemisphere (such as when transfer is required) overall efficiency declines.
Recognition of incomplete and distorted figural-pictorial information PC was shown in full field, a series of 20 pictures depicting 10 objects or animals (for example a boot, airplane, rabbit, fish). He was given two trials per stimulus, the second trial consisting of the same stimulus as the first trial but containing more visual information. This unpublished test (Joseph) is scored such that correct responses on trial 2 receive 5 points. Normal or average performance is indicated by a score of 70 or more (N=47 neurologically intact males and females) and it has been found that individuals with right hemisphere injuries tend to score below 50 (N=84). However, left parietal and parietal-temporal (inferior) injuries also disturb performance on this test (N=18), with scores ranging from 50-70. PC received a score of "0", which indicates a severe disturbance in the capacity to perform operations requiring visual closure and the formation of a visual-spatial pictorial gestalt.
In addition, PC was administered the Hooper Visual Organization task both pre- and post-operatively. This task involves the recognition of distorted figures (30 total). Normal or average performance is indicated by a score of 25 and above. Pre- and post-operative performance was essentially identical, PC receiving scores of 13 and 12 respectively (moderate level of disturbance). As noted, the Wechsler Adult Intelligence Scale was administered to PC, and he obtained a Performance (non-verbal, visual-spatial) IQ of 86 (16% rank) pre-operatively and a Performance IQ of 78 (7% rank) post-operatively. This indicates that over 84% of the normative population scores better than PC on these measures. Hence, in general, capacities most often associated with normal or average right hemisphere functioning are moderately to moderately-severely reduced.
DISCUSSION
Although ostensibly right hand dominant for most motor activities and writing, the patient largely lost his ability to use the right extremity for these tasks following callosotomy (thereby disconnecting the parietal-temporal-occipital regions of the left and right hemisphere). In contrast, when assessed two weeks following surgery PC demonstrated (much to his surprise) a left hand dominance for language related operations, including writing and the ability to perform tasks requiring temporal sequencing. This is a reversal in dominance as contrasted with the majority of right handed individuals in whom the left hemisphere mediates not only language, but the ability to analyze temporal sequences or perform/program serial or sequential hand/finger movements.
Similarly, as noted via the patient's performance on standard dichotic listening tasks, the sodium amytal study, and the tachistoscopic study involving words and digits, the left cerebral hemisphere appears to have little expressive or receptive linguistic ability. Hence, PC failed to respond when the left hemisphere was stimulated, but was able to speak, comprehend, and correctly identify and describe pictorial stimuli (that is words, digits, pictures), as well as report dichotic stimuli presented to the right cerebral hemisphere. Moreover, it is of not that although PC could write to a limited degree with the right hand following the callosotomy, when blindfolded his ability to use the right (but not left) hand for these tasks was largely abolished.
It thus appears that before operation, the posterior callosal pathways were involved in transmitting linguistic information organized by the temporal-parietal regions of the right hemisphere to the motor areas of the left cerebrum which subserved hand usage. Hence, following callosotomy, the patient subsequently demonstrate difficulty when required to write/spell concrete and abstract words with the right hand and lost this ability when blindfolded. In contrast, when blindfolded, the left hand made a single error of omission. Thus, presumably, when the posterior callosal interconnections were severed, PC became almost completely dependent on external visual cues (available to both hemispheres) when using the right hand for linguistic operations.
In contrast, when required to spell emotional words, PC's difficulty with right hand usage abated, and a distinct right hand advantage over the left re-emerged. The right was also superior to the left hand when required to match emotional intonation (prosody) to appropriate facial (pictorial) emotional stimuli. Moreover, the left hand responded more slowly when writing emotional vs natural words of equal length and frequency of occurrence. Hence, when stimuli were emotional right hand (left hemisphere) performance was augmented. Hence, overall, in contrast to the majority of right handed individuals, among whom the right hemisphere has been shown to be dominant in processing and expressing emotional stimuli, PC demonstrated a significant reversal in functional asymmetry such that his left hemisphere has come to subserve the mediation of emotional stimuli and related information.
Presumably these significant reversals in hemispheric mediation of language and emotion are secondary to early cerebral damage, functional reorganization, competitive "crowding" and thus the subsequent displacement of "limbic" and other synaptic fiber processes which in seeking neocortical representational space grow into "vacant" areas within the left hemisphere "normally" committed to language. In that vocabulary and grammar are in part an outgrowth of and strongly related to "limbic" or prosodic-melodic and emotional speech it would seem that both hemispheres contain neuronal substrates which can subserve "language". As such, the possibility or potential for reversed representation is enhanced.
In addition, significant reversals were also noted in regard to tactile and somesthetic perceptual functioning. PC reported a loss of sensation in the left extremities following surgery (which was confirmed via neurological and neuropsychological examination), and demonstrated difficulty recognizing textured stimuli presented to the left hand or localizing information transferred to the left extremity. Stereognostic deficiencies were also observed when the left hand was assessed. In that a number of investigators have reported that the majority of individuals studied demonstrate a right hemisphere dominance in regard to many aspects of somesthetic and stereognostic functioning, these results indicate a significant reversal in lateralized representation of these capacities; that is PC shows a left hemisphere dominance which in turn is possibly due to the availability of appropriate terminal substrate.
Both before and after callosotomy, PC was found to be moderately impaired when required to perform tasks involving visual-spatial analysis and perceptual organization functioning, a finding that has been frequently reported as characteristic of individuals who acquire right hemisphere language secondarily due to early left hemisphere injury. Presumably this is a function of "crowding" and the lack of representational space for these processes within the left cerebrum. On the other hand, perhaps complex visual-spatial processing requires the dual and shared activity of both cerebral hemispheres. In this regard five full "split" callosotomy patients examined in this laboratory have shown similar deficits, particularly in regard to the ability to form visual closure (Joseph, unpublished observations).
The overall results demonstrate a notable reversal in functional and lateralized asymmetry in this right-hand dominant individual. The right hemisphere has come to subserve linguistic and temporal-sequential information analysis, whereas the left cerebrum has become responsible for the mediation of somesthetic and emotional functions. However, PC, like ten other right hemisphere language dominant individuals we have examined, has retained left hemisphere dominance for handedness. Why handedness does not necessarily follow language and its supporting temporal-sequencing functions to the right hemisphere in these cases is unknown. Possibly, differential functional sparing and reorganization is partly due to relative differences in neocortical and subcortical plasticity during early development. Lesion site is also possibly an important differential contributor.
REFERENCES










