





Dual Mental Functioning In a Split-Brain Patient (reprinted from the Journal of Clinical Psychology, 44, 770-779, 1988).
Rhawn Gabriel Joseph, Ph.D.
Yale University Medical Center Seizure Unit, Dept. of Neurology, West Haven, V. A. Medical Center, Dept. of Neurology.
ABSTRACT Case studies of two individuals who had undergone complete corpus callosotomies are presented. In addition to anecdotal observations, controlled neurobehavioral and neuropsychological testing indicated that although both patients demonstrated the disconnection syndromes unique to "split-brain" patients, they also differed rather dramatically. For example, 1-C's left hemisphere developed bilateral motor control, whereas 2-C demonstrated the presence of two independent forms of conscious- awareness, one of which resided in the right and the other in the left hemisphere. Hence, 2-C's right brain was capable of gathering, understanding, recalling, and expressing (non-verbally) various forms of information as well as directing independent behavioral activity as manifested by his left extremities. Indeed, 2-C's left arm and leg not only engaged in cont- rolled, directed, and purposeful behavior, but at times performed activities which his left hemisphere found objectionable and annoying. In some instances, physical struggles involving the right and left extremities of this patient were observed. In contrast, 1-C's right hemisphere appeared to be lacking in higher level cognitive capabilities. Speculations regarding mental activity and hemispheric laterality are presented.
"Everything we have seen indicates that the surgery has left these people with two separate minds, that is, two separate spheres of consciousness. What is experienced in the right hemisphere seems to lie entirely outside the realm of awareness of the left hemisphere. This mental division has been demonstrated in regard to perception, cognition, volition, learning and memory." -Sperry (1966, p. 299)
In the normal brain it has sometimes been supposed that mental unity is supported and maintained via the extensive bridge of nerve fibers which interconnect the right and left cerebral hemispheres; i.e. the corpus callosum, and that only in conditions such as following callosotomy, does something akin to a splitting of the mind occur (cf Puccetti [Open Peer Commentary], 1981). Nevertheless, common experience seems to argue otherwise, for it often occurs that people will express certain behaviors, act on various impulses, make "thoughtless", embarrassing statements or a "slip of the tongue" and "have no idea" as to "what came over" them. In some instances they may even fail to become aware that anything unusual or objectionable has resulted, or conversely, conjure up explanations for their actions (Joseph, 1980, 1982, 1986a; Nisbett & Wilson, 1977). Similar anomolies confront us in regard to certain emotions, desires, impulses, and conflicts --the origins and source of which are seemingly submerged and hidden; at least from the language dominant hemisphere (i.e. in most instances the left).
Indeed, in some situations one brain half may have little or no knowledge as to what is occurring in the other (Geschwind, 1965; Joseph, 1980, 1982; 1986a). Presumably this is a consequence of lateralized specialization. Some forms of information cannot be transferred or even recognized by the opposite hemisphere (Galin, 1974; Geschwind, 1965; Joseph, 1982).
This inability of the left hemisphere to fully recognize or linguistically code certain forms of emotional and non-linguistic information has in turn greatly added to the belief that such stimuli originate and are expressed "unconsciously" (Galin, 1974; Joseph, 1980, 1982; Miller, 1986). However, rather than unconsciously motivated, many of these reactions and feelings are controlled and expressed by the right hemisphere without the aid or linguistic knowledge of the left (Joseph, 1980, 1982).
When the left hemisphere is denied access to information retained or processed by the right, and/or is unable to learn why a certain behavior or action was initiated, it typically makes up explanations (which it believes) or engages in active denial (Gazzaniga & LeDoux, 1978; Geschwind, 1965; Joseph, 1980, 1982, 1986a,b; Joseph, Gallagher, Holloway, & Kahn, 1984; Risse & Gazzaniga, 1980). For example, it is well known that with severe right cerebral injuries a patient (or rather his/her left hemisphere) might ignore the left half of the body, and even deny ownership of the left arm or leg. If the ignored left hand is shown to them they may claim it belongs to the doctor or a person in the next room (see Joseph, 1986a, for review).
In fact, since unilateral neglect and denial are often association with lesions of the right hemisphere whereas similar disturbances are rare following left cerebral damage, it appears that the right hemisphere may maintain a greater or even bilateral awareness of the body-environmental continuum (Geschwind, 1981; Heilman & Van Dan Abel, 1980; Joseph, 1982, 1986a). Thus, when the left brain is damaged, the right attends to both halves of body-space and there is no neglect. The left hemisphere, in contrast, is more restricted such that (linguistic) consciousness and attentional functioning are limited to contralateral body-space.
My purpose in raising these issues is to present some observations regarding two different individuals with complete callosotomy (i.e. "split-brains"), one of whom demonstrated left sided spatial-conceptual neglect (when his left hemisphere was tested), as well as the presence of two expressively independent forms of conscious-awareness. Indeed, following callosotomy, this patient (2-C) was frequently confronted with situations where his left extremities not only acted independently, but engaged in purposeful and complex behaviors --some of which he (or rather, his left hemisphere) found objectionable and annoying.
For example, 2-C complained of instances where his left hand would act in a manner completely opposite to what he expressively intended, such as turn off the T.V., or change channels, even though he (or rather his left hemisphere) was enjoying the program, or perform socially inappropriate actions (e.g. attempting to strike or even strangle a relative). On at least one occasion, his left leg refused to continue "going for a walk" and would only allow him to return home.
In the laboratory, he often became quite angry with his left hand, striking and expressing hate for it. Several times his left and right hands were observed to actually engage in physical struggles. For example, following the application of two different fabrics to his hands (e.g. sandpaper to the right, wire screen to the left) while both were hidden from view (and without him being informed that the materials were different), although he correctly pointed with the left to the fabric applied, he grabbed his left with his right hand and attempted to force it to point to the material experienced by the right hand. His left hand, however, resisted and continued to point to the correct material. In these instances there could be little doubt that his right hemisphere was behaving with purposeful intent and understanding whereas his left brain had absolutely no comprehension as to why his left hand (right hemisphere) was behaving in this manner.
CASE DESCRIPTIONS
2-C. Patient 2-C had his first seizure at age eight and frequently suffered from complex partial seizures as well as status epilepticus (with up to 100 seizures per day ) several times per month. These were often accompanied by secondary generalization. Medication proved to be of little usefulness in controlling this activity.
Prior to surgery (at age 20) EEG and depth electrodes demonstrated many right frontal events which led to bilateral synchronous seizure activity. Independent discharges were noted throughout the left cerebrum. CT-scan failed to indicate the presence of any gross lesions. The patient was of low average intelligence (WAIS), and sodium amytal ("Wada test") indicated left hemisphere dominance for speech.
Following callosotomy neurological examination was remarkable for extinction and suppression of the left visual field and left half of the body (when verbal reports were required). At this time the patient began to comment upon independent behavioral activity initiated by the left hand which he could not control. It was noted by the examining physician that his left arm and leg would not consistently follow commands and/or would respond in a maner opposite to what was requested.
Unfortunately, although reduced, the patient continued to experience some seizure activity. EEG indicated moderate generalized slowing with bilateral spike and wave and poly spikes which occurred both independently and dependently. During a seizure the EEG indicated right cerebral onset with rapid generalization. This condition remained basically unchanged up to the time he was evaluated by this examiner, 3-years post surgery (at age 23).
1-C. Patient 1-C developed complex partial seizures at about age 4 which became progressively more difficult to manage despite the use of multiple medications. His seizures were characterized by left-sided head turning with tonic posturing of the left extremities. Up until the time of his first initial surgery (i.e. partial callosotomy of the body and rostrum) he was experiencing several seizures a day. Prior to surgery EEG was consistently abnormal with frequent bilateral spikes and poly spike discharges in the frontal regions. Slowing of the right posterior temporal region as well as independent left and right frontal and right occipital spikes were noted. Sodium amytal assessment indicated left hemisphere speech.
Five months post initial surgery 1-C underwent a complete callosotomy. Frequency of seizures were significantly reduced. EEG was essentially indentical to that seen prior to surgery. Neurological exam indicated good bilarteral motor control although left sided extinction and neglect of the left visual field was noted initially when verbal reports were required.
POST OPERATIVE NEUROBEHAVIORAL/NEUROPSYCHOLOGICAL EXAMINATIONS
SOMESTHESIS: Touch sensation and localization was adequately appreciated when applied to the right half of either patient's body. When applied to the left half, 1-C responded correctly on 30% of the trials (i.e. indicating if he was touched), wheras 2-C responded with 0% accuracy when verbal reports were required. However, when the patient was required to simply raise the left hand when the left half of the body was touched, 1-C continued to respond correctly on only 30% of the trials whereas 2-C now responded correctly on 90% (10 trials per body half).
STEREOGNOSIS: When common objects were placed in the right hand, both 1- and 2-C named them without difficulty. When placed in the left hand neither patient was able to name correctly; nor were they able to indicate, verbally or with the right hand (via pointing) the correct object when offered multiple (visual) choices. When asked to point with the left hand, 1-C responded correctly on 1 of 10 trials whereas 2-C responded with 90% accuracy.
When required to palpate complex geometric shapes and to then find a similar shape among several differing in size and thickness, both responded with 100% accuracy when palpating and choosing with the right hand (20 trials total). However, 1-C responded with 40% accuracy using the left, whereas 2-C responded with 80% accuracy. When required to palpate with the right and choose with the left (i.e. interhemispheric transfer), 1-C scored with 20% and 2-C with 10% accuracy (less than chance). Transfer from left to right resulted in 45% accuracy for 1-C whereas 2-Cs performance remained unchanged (10%).
Hence, 1-C appears capable of transferring some tactile information between the hemispheres (which may have been mediated by ipsilateral pathways) whereas performance by his left hand was actually quite poor. In contrast, 2-C, although failing to demonstrate transfer, proved capable of responding appropriately with his left hand (right brain).
DIFFERENTIAL SIMULTANEOUS TACTILE STIMULATION. This task (described in detail by Joseph, 1986b; Schwartz, Marchok, Kreinick, & Flynn, 1979) involved simultaneously stimulating both hands (while out of view) with either the same or two different textured materials (e.g. sandpaper to the right, velvet to the left) and required the patient to point (with the left and right hand simultaneously) to an array of fabrics hanging in view on the left and right of the testing apparatus . Hence, following stimulation the patient would pull his hands out from inside the apparatus and point with the left to the fabric felt by the left, and with the right to the fabric felt by the right.
1-C consistently demonstrated left extremity suppression such that he would point with his left and right hand only to the fabric applied to the right. In contrast, 2-C failed to demonstrate suppression and almost consistently pointed with the left hand to the fabric experienced by that extremity.
Suprisingly, when 2-C was stimulated with two different fabrics, although his left hand (right hemisphere) responded correctly, his left hemisphere vocalized: "Thats wrong!" Repeatedly he reached over with his right hand and tried to force his left extremity to point to the fabric experienced by the right (although the left hand responded correctly!). His left hand refused to be moved and physically resisted being forced to point at anything different. In one instance a physical struggle ensued, the right grappling with the left.
Moreover, while performing this (and other tasks), 2-C made statements such as: "I hate this hand", or, "this is so frustrating", and would strike his left hand with his right or punch his left arm. Hence, it was readily apparent that 2-Cs left hemisphere had no idea that his left hand was responded correctly or why his right brain was behaving in that manner. Not once, however, did his left hand attempt to interfere with the choices made by the right.
UNILATERAL VS WHOLE BODY MOVEMENTS TO COMMAND: Each patient was presented with a series of 10 unilateral (e.g. "salute like a soldier") or 10 whole body commands (e.g. "stand like a boxer"). Overall, 1-C responded appropriately to over 90% of the left or right unilateral or whole body commands with no left vs right discrimination errors.
In contrast, 2-C was able to respond correctly to all commands involving the right body but to only 3 of the 10 whole body commands. When asked to perform body movements with the left extremities (e.g. "point to your left ear with your left hand"), 2-C was unable to consistently perform correctly as he made incorrect or no movements of the left extremities. In these instances, 2-C again remarked that he hated the left half of his body.
VISUAL SPATIAL SKILLS: IN full visual field both patients were shown a series of 20 incompletely drawn figures (requiring visual closure for identification) of 10 objects or animals, e.g. a boot, fish, etc. There were two trials per stimulus, the second containing more visual information. Average performance is indicated by a score of between 70-100 (Joseph, unpublished, "The Incomplete Figures Test"). 1-C received a score of 25 and 2-C a score of 10 indicating that both (or at least their left brains since a verbal response was required) suffer from severe disturbances in the ability to perform closure and form a visual gestalt.
The Hooper Visual Organization tests was also administered. This involves the recognition of distorted figures (30 total). Average performance is indicated by a score of 25 and above (Hooper, 1957). 1-C received a score of 21 and 2-C a score of 22, indicating reduced levels of functioning.
Both patients were found to have left sided visual field cuts when verbal responses were required. However, when asked to raise their left hand when they saw the experimenters fingers wiggle, 1-C failed to respond whereas 2-C responded correctly on 6 of 10 trials when stimulated to the left of visual midline.
Both were also required to draw and copy several geometric forms and objects (e.g. a flower) as well as a clock with all the numbers. 1-C was able to adequately copy and spontaneously produce various forms, including 2-dimensional shapes involving perspective. In contrast, the spontaneous drawings and copies of 2-C were distorted, macrographic, and he was unable to reproduce figures involving perspective with his right hand. His left hand would not consistently cooperate on these tasks. Left sided neglect and inattention were also noted in his drawings. For example, his clocks were drawn such that all the numbers appeared on the right half of the figure .
RESPONSES TO T-SCOPE VISUAL-PICTORIAL STIMULI:
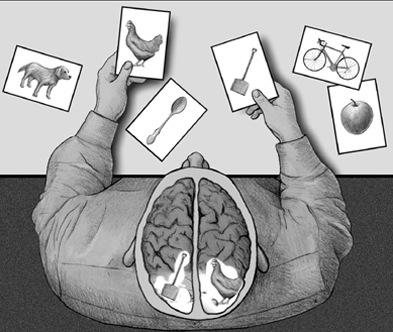
Following the procedures and rationale outlined in detail elsewhere (Joseph, 1986b), the right and left cerebral hemispheres of both patients were separately and individually presented, via tachistoscope, with 40 visual-pictorial scenes (e.g. a boy with a ball, a man with an umbrella), 20 written words (e.g. "Hat"), and 10 digits. All were presented 3 degrees to the left or right of visual midline for 150 msec. Visual field presentation order was counterbalanced and each stimulus was presented twice, once to each visual field. The patients were required to describe the pictures and to verbalize the words or digits presented.
Both responded with 100% accuracy when the right visual field (left hemisphere) was stimulated. When the left visual field (right hemisphere) was stimulated, regardless of the stimulus presented, 1-C failed to respond correctly. When presented with written words and allowed to guess by pointing with his left hand to one of 4 words presented in full field, he responded correctly 3 times (i.e. at about the level of chance).
When 2-Cs right hemisphere was presented with visual-pictorial material, he was able to provide verbal responses and in all cases correctly described some aspect of what was viewed. In many cases, the responses made following right hemisphere presentation were almost identical to those following left cerebral stimulation. However, 12 of the 40 responses made following T-scope presentation to the right brain were wildly confabulatory and sometimes marked by perseveration. For example, when shown a picture of a man walking in the rain and carrying an umbrella, although his left cerebral responses were accurate, following right cerebral presentation he replied: "A pizza man making a pizza at a pizza joint".
Of the 20 words presented to the right hemisphere, 2-C responded correctly on 40% of the trails. Later, when 10 of the same words were again presented to the right brain and he was allowed to guess by pointing with his left hand to words presented in full field, he responded correctly 8 times (80%). He was able to name 4 of the digits presented to the left visual field (40%).
RECOGNITION OF ENVIRONMENTAL SOUNDS. Each patient was presented via tape recording, with 20 sounds from the environment (e.g. crickets chirping, rain and thunder). Each sounds was presented once for approximately a 2 second time period. It has been reported that the right cerebral hemisphere is dominant for recognizing non-verbal and environmental sounds (Blumstein & Cooper, 1974; Curry, 1967; Knox & Kimura, 1970). On this task (Joseph, Note 1, Environmental Sounds Test), individuals with right frontal-temporal damage tend to perform quite poorly (with 5 or more incorrect responses), whereas neurologically intact individuals (N=24) respond with 90-100% accuracy.
1-C made 8 errors (60% correct) in verbally identifying these sounds. Similarly, 2-C was correct on only 12 of the trials (60% correct).
DISCUSSION
Following complete callosotomy both 1- and 2-C displayed the disconnection syndromes unique to commissurotomy patients (Bogen, 1979; Gazzaniga & LeDoux. 1978; Sperry, 1966). Hence, when tactually stimulated on the left side of the body, (the left hemisphere's of) both patients demonstrated marked neglect when verbal responses were required, were unable to name objects placed in the left hand, and failed to report the presence of a moving stimulus in the left half of their visual fields. In addition, both demonstrated marked difficulties naming incomplete figures (and thus forming visual closure) as well as a reduced ability to name and identify non-linguistic and environmental sounds --capacities associated with the functional integrity of the right hemisphere (which was not afforded an opportunity to respond in this series of tests).
Both patients, however, also differed rather dramatically. For example, by raising his left hand, 2-C's right brain was able to indicate when he was tactually or visually stimulated on his left side. When tachistoscopically presented with words to the left of visual midline, although unable to name them, when offered multiple visual choices in full field his right hemisphere was able to point correctly with the left hand to the word viewed. With his left hand 2-C was also able to respond correctly on 90% of the texture identification trials and resisted attempts by his right hand to make it point elsewhere.
Surprisingly, when visual-pictorial material were tachistoscopically presented to his right hemisphere, 2-C in many instances was able to describe what was viewed. Many of his descriptions, however, were characterized by wild confabulatory responses (e.g. describing a man with an umbrella as a man making a pizza). As discussed in detail elsewhere (Joseph, 1986a; Joseph, et al, 1984) confabulation is often the result of incomplete information transfer from the right to left hemisphere (sodium amytal indicated left hemisphere dominance for expressive speech in both patients). In contrast, 1-C was unable to provide responses when his right hemisphere was presented with pictures, words or numbers --even when offered multiple choices and the opportunity to point with his left hand.
In addition these two patients significiantly differed in the degree of bilateral motor control exhibited by the left hemisphere. Hence, 1-C was largely able to program and control the left half of his body, such that in response to verbal commands he correctly performed whole body, unilateral, as well as commands involving movement across the body midline. He also showed some (left cerebral ) consciousness of stimuli applied to his left side. In contrast, 2-C frequently experienced and demonstrated difficulty making the left half of his body respond to verbal and left hemisphere mediated commands.
Indeed, the functional and expressive independence of 2-Cs right cerebrum caused this individual (or at least his left hemisphere) a considerable degree of frustration, anger and embarrassment. In this regard he complained of situations where his left extremity would turn off or change chanels on the T.V. (even though he, i.e., his left hemisphere was enjoying the program), refuse to walk in certain directions, act in a manner completely opposite to what he expressively intended, or perform socially inappropriate actions (such as attempting to strike a relative).
In the laboratory, on several occasions, he became angry with his left hand, swore and expressed "hate" for it, struck his left hand/arm with his right hand, and engaged in physical struggles with his left extremity, the right attempting to force the left to comply with some particular activity or to cease to act in a manner which the left hemisphere found objectionable or annoying. In many (if not most) instances, the left resisted and continued to behave in the manner directed by the right hemisphere.
In general, these findings indicate the isolated right cerebral hemisphere of 2-C was able to understand and follow certain simple verbal commands, obtain and maintain knowledge of various visual, auditory, lingustic, and somesthetic events, as well as respond, make decisions and act purposefully --even when his left hemisphere had no idea as to what information the right possessed and why it was behaving in a particular manner.
Given the differential behavioral observations regarding the activity and responsiveness of the left half of their bodies, it appears that 2-C (unlike 1-C) is possessed of two minds, one of which resides within the right, the other within the left cerebral hemisphere. Nevertheless, it appears that 2-Cs left hemisphere remains predominant in regard to most expressive activities.
The kind of independent sometimes obstinent and mischievous behavior demonstrated by 2-Cs right hemisphere is not rare and has been observed in other callosotomy patients. In its most subtle manifestations the disconnected right hemisphere may attempt to aid the left or provide it with cues when the left (speaking) brain is called upon to describe or guess what type of stimulus has been shown to the right (such as in a T-scope experiment). This may involve the right brain nodding the head, clearing the throat (so as to indicate to the left brain that it has guessed incorrectly) or by attempting to trace or write (with the left) an answer on the back of the right hand (e.g. Sperry, Zaidel & Zaidel, 1979).
Nevertheless, the behavior of the right hemisphere is not always cooperate, and like 2-C above, sometimes it engages in behavior that the left brain finds objectionable, embarrassing, puzzling, mysterious, and/or quite frustrating. This is probably true for the normal as well as the "split-brain" individual.
For example, Akeleitis (1945) describes two patients with complete corpus callosotomies who experienced extreme difficulties making the two halves of their bodies cooperate. "In tasks requiring bimanual activity the left hand would frequently perform oppositely to what she desired to do with the right hand. For example, she would be putting on clothes with her right and pulling them off with her left, opening a door or drawer with her right hand and simultaneously pushing it shut with the left. These uncontrollable acts made her increasingly irritated and depressed" (Akeleitis, 1945, p. 595).
Another patient experienced difficulty while shopping, the right hand placing something in the cart and the left hand putting it right back again. Both patients frequently experienced other difficulties as well . "I want to walk forward but something makes me go backward". A recently divorced male patient noted that on several occassions while walking about town he found himself forced to go some distance in another direction. Later (although his left hemisphere was not conscious of it at the time) it was discovered (by Dr. Akeleitis) that this diverted course, if continued, would have led him to his former wife's new home.
Geschwind (1981) reports a callosal patient who complained that his left hand on several occasions suddenly struck his wife--much to the embarrassment of his left (speaking) hemisphere. In another case, a patient's left hand attempted to choke the patient and had to be wrestled away (Goldstein, 1908; cited by Geschwind, 1981).
Brion & Jedynak (1972; cited by Geschwind, 1981) indicate that this type of independent left sided (right hemisphere) activity was common in their split-brain patients and termed it "la main entragere" -i.e., the alien hand.
Although it is impossible to determine which patient (1- or 2-C) actually more closely approximates the conditions characteristic of the "normal" cerebrum (insofar as dual mental functioning is concerned), the neglect phenomena demonstrated by 2-C's left brain certainly most closely approximates the performance of individuals who have suffered a loss of right cerebral input, as well as the models of dysfunction (regarding neglect) advanced by a number of investigators. Hence, although 2-C retained the ability to orient and attend to his left side such as when the left half of his body was "misbehaving" the spontaneous drawings and copies made by his left hemisphere showed a greater degree of left vs right distortion, as well as frank left sided neglect (see Figure of clock). Thus conceptually, cognitively, and consciously, his left cerebrum tended to ignore the left half of space and to deny events experienced and expressed by the right hemisphere.
Possibly (in contrast to 2-C), 1-C's overall performance, bilateral motor control and lack of demonstrable right cerebral mental activity is due to functional reorganization stemming from the early onset of his brain injuries and seizure disorder (cf Joseph, 1986b). Thus, it is noteworthy that 1-C first developed seizures at age 4, vs age 8 for 2-C.
For example, it is possible that following early right cerebral injury the capacity for mental duality is diminished. Hence, rather than the right brain taking over left hemisphere functions (as sometimes occurs with early left cerebral damage, e.g. Joseph, 1982, 1986b), some right brain functional capacities, in 1-C's case, were acquired by his left hemisphere. Hence, we find that, as compared to 2-C, 1-Cs left hemisphere developed a considerable degree of bilateral motor control and a limited capacity to receive tactile-motor information normally destined for the right cerebrum. In addition, his left hemisphere was able to perform some simple tasks associated with the functional integrity of the right hemisphere (e.g. visual-spatial, constructional, etc.). In contrast, as pertaining to higher order cognitive capacities, such as perceiving, analyzing and recognizing complex visual-pictorial stimuli, or simple written words, the right hemisphere of 2-C was clearly superior to 1-C's right brain.
These differential finding raise the possibility that in some cases (such as 1-C) there may in fact be "nobody home" insofar as right hemisphere awareness and other functioning is concerned, such that by "default" the left cerebrum comes to control (to a limited extent) faculties commonly mediated by the right (e.g. due to early injury).
Overall, given the independent neurobehavioral, cognitive, and psychological activity manifested by 2-Cs right hemisphere, the tendencies of his left hemisphere to forcefully attempt to control this activity and it's lack of knowledge concerning the origins or motivations governing the behavior of the right, as well as the other issues discussed above, the possibility is certainly raised that "normal" brain functioning may be characterized by similar interactions. That is, in some instances, the right cerebral hemisphere may purposefully initiate behavior, guide response choices and emotional reactions, as well as recall and act upon certain desires, impulses, situations, or environmental events --without the aid, knowlesge, or active (reflective) participation of the left.






